

Abstract
Background: Proteasome inhibitors (PI) represent an important therapeutic advance in the treatment of patients with relapsed/refractory multiple myeloma (RRMM). In 2017, three distinct PIs (bortezomib [BTZ], carfilzomib [CFZ] and ixazomib [IXA]) were available in Germany but real-world data describing their usage was scarce.
Aim: To describe characteristics and treatment experience of PI-treated patients with RRMM in Germany.
Methods: A national retrospective medical chart review included consecutive patients treated with at least one dose of PI-based regimen in participating hospitals/centers across Germany between January and June 2017. The following data were extracted until April 2018 or death of patient, whichever occurred first: patient demographics, disease characteristics and treatment history at diagnosis and at initiation of PI-based therapy. Physician assessed treatment response were also collected.
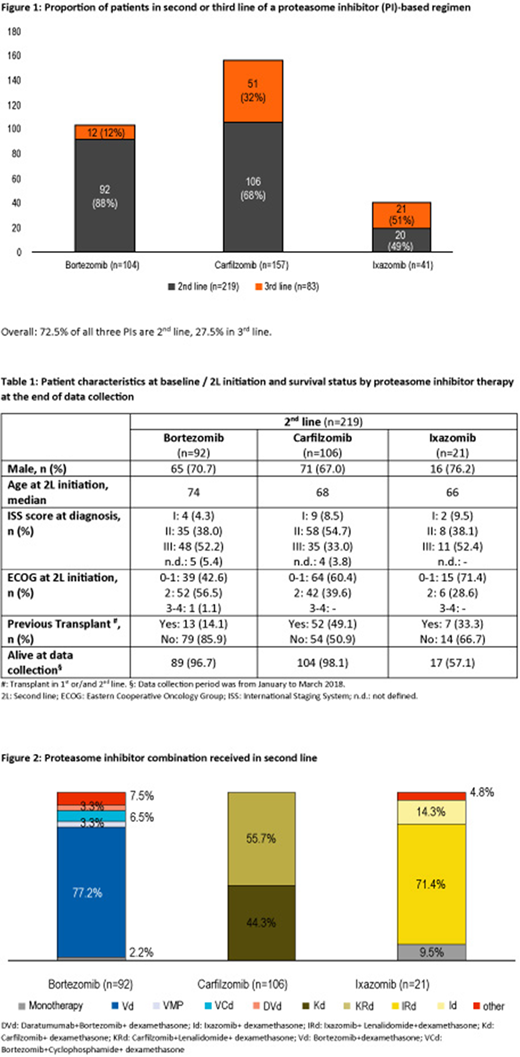
Results: Physicians from 44 participating centers extracted 302 patient charts, including 219 patients in 2nd line (2L) and 83 in 3rd line treatment (3L), as shown in Figure 1. Results for 2L patients are described below (Table 1, Figure 2):
BTZ-treated patients represented 42% of patients (n=92) with a PI-based therapy in 2L. BTZ was often combined with dexamethasone (dex) alone (77%). Median age was 74 years and 56.5% had an ECOG status ≥2 at 2L initiation. Most patients (86%) did not receive a prior transplant. Median treatment duration was 6 months among 40 patients who completed 2L; based on 38 narratives, 2L was ended as planned (47.4%). Where response was available (n=83), 25% of patients achieved a complete response/very good partial response [CR/VGPR]. Median time to next treatment (TTnT) was 7.5 months for 12 patients who moved to 3L. Patient profiles differed in terms of prior treatment exposure: 22% of patients had been treated with a BTZ-based therapy in both 1L and 2L and 62% switched therapies from 1L lenalidomide (len) to BTZ. None of the patients receiving len in 1L were transplanted. A CR/VGPR was achieved by 65% of prior BTZ-treated patients (13/20) and 30% of patients with prior len therapy (17/57).
CFZ-treated patients: 48% (n=106) of patients received CFZ-based therapy in 2L. Of those, 56% (n=59) received CFZ in combination with len/dex (KRd) and 44% (n=47) with dex alone (Kd). Median age was 68 years, 60.4% had an ECOG status of 0-1 at 2L initiation and 49% had received a transplant. In 1L, 82% had received a BTZ-based regimen. Where response was mentioned (n=89), a CR/VGPR was reached in 53% of CFZ-treated patients. Median treatment duration was 6.5 months (24/106). Based on 21 narratives, the main reason for discontinuing CFZ in 2L was disease progression (47.6%). Median TTnT was 9.5 months for 10 patients who moved to 3L. The patient profiles by KRd or Kd combination were as follows: at KRd initiation, median age was 65 years, 10.2% of patients had an ECOG status ≥2 and 72.9% were transplanted. At Kd initiation, median age was 71 years, 76.6% of patients had an ECOG ≥2 and 19.1% were transplanted.
IXA-treated patients (n=21) represented only 10% of PI-treated patients in 2L. Median age was 66 years, 71.4% had an ECOG status of 0-1 at 2L initiation, 33% were transplanted, and 72% had received a BTZ combination in 1L. Information on response was premature as it was only available for 13 patients with no CR reached (VGPR 77%). Median treatment duration was 4 months (n=9) and median TTnT was 10 months for 4 patients who moved into 3L.
Limitation: The main limitation of the study was the sample size of IXA-treated patients due to open inclusion criteria to select patient charts. This analysis was not powered to compare between PIs. Hence, results are descriptive of the clinical experience with PI-based therapy to date and reflect current treatment practices in Germany in 2017.
Conclusion: In Germany, distinct patient characteristics are observed in clinical practice by selected PI-based therapy. Patients treated with novel PI agents in 2L are generally younger and more transplanted than bortezomib-treated patients; these appear to be important considerations when tailoring therapy in RRMM. In addition, the choice between triplet or doublet therapy for CFZ-based combinations seems to reflect prior transplant status and patients' overall functional performance. Evidence suggests that use of novel PI agents such as CFZ can translate into deeper response in 2L.
Steinmetz:Amgen, Celgene, Novartis, Vifor: Research Funding; Amgen; BMS, Celgene, Hexal-Sandoz, Medice, Novartis; Janssen-Cilag; Pharmacosmos; Pfizer, Vifor; Ariad: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Alexion, Amgen, Bayer, Celgene, Janssen-Cilag, Novartis: Other: Travel grants. Singh:Amgen: Employment, Equity Ownership. Lebioda:Amgen: Employment, Equity Ownership. Mantonnier:Kantar Health: Employment, Other: Received funding to conduct this research. Fink:Kantar Health: Employment, Other: Received funding to conduct this research. Rieth:Amgen: Employment, Equity Ownership. Suzan:Amgen: Employment, Equity Ownership. Gonzalez-McQuire:Amgen: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal